I'm a 35 year old microbiologist and molecular biologist with systemic mastocytosis, Ehlers Danlos Syndrome, Postural Orthostatic Tachycardia Syndrome, Adrenal Insufficiency, and an assortment of other chronic health issues. My life is pretty much a blast.
Inhibits many inflammatory molecules, like TNF, IL-8, MCP-1, IL-1b, IL-6, CRP, IL-12, VCAM-1, MMP2, MMP9, GM-CSF and IL-17
Opposes action of leptin, a mast cell mediator
Level is increased by lack of sleep, promoting excessive hunger.
Hirayama T, et al. Ghrelin and obestatin promote the allergic action in rat peritoneal mast cells as basic secretagogues. Peptides 2010: 31(11), 2109-2113.
Baatar D, et al. The effects of ghrelin on inflammation and the immune system. Molecular and Cellular Endocrinology 2011: 340(1), 44-58.
Glucagon
Pancreas
Regulates amount of available glucose
Triggers breakdown of glycogen and production of glucose in liver, raising blood sugar
Released when blood sugar is too low
Can increase level of cAMP in myocardium to overcome effect of beta blockers
Anecdotal reports that glucagon may be able to relax esophagus sphincter to pass impacted food
In anaphylaxis patients on beta blockers, glucagon can be used to reduce resistance to epinephrine and increase blood pressure
May be considered to treat Kounis Syndrome where epinephrine is contraindicated
Histamine H3 receptor may regulate glucagon release from pancreas
Nakamura T, et al. Role of histamine H3 receptor in glucagon secreting aTC1.6 cells. FEBS Open Bio 2015: 5, 36-41.
Thomas M, Crawford I. Glucagon infusion in refractory anaphylactic shock in patients on beta blockers. Emerg Med J 2005: 22, 272-276.
Glucagon-like peptide 1 (GLP-1)
Small intestine
Increases release of insulin and nausea
Decreases release of glucagon, desire to eat and amount of food consumed
Increases anxiety
Possible relationship between GLP-1 and histamine in the brain, but still unclear
GLP-1 level is modulated by leptin, a mast cell mediator Increases ACTH and cortisol
Gotoh K, et al. Glucagon-like peptide-1, corticotropin-releasing hormone, and hypothalamic neuronal histamine interact in the leptin-signaling pathway to regulate feeding behavior. FASEB J 2005: 19(9), 1131-1133.
Gonadotropin releasing hormone
Hypothalamus
Stimulate FSH and LH release from pituitary
Part of HPG axis
Drive secondary sex characteristics
Regulate sex hormone release
Histamine induces GnRH release in some studies
Noris G, et al. Histamine directly stimulates gonadotropin-releasing hormone secretion from GT1-1 cells via H1 receptors coupled to phosphoinositide hydrolysis. Endrocrinology 1995: 136(7), 2967-2974.
Growth hormone releasing hormone
Hypothalamus
Stimulate growth hormone release from pituitary
Regulates bone growth
Regulates metabolism of proteins, carbohydrates and lipids
Induces mast cell degranulation and release of serotonin and histamine, causing low blood pressure
Macia RA, et al. Hypotension induced by growth hormone releasing peptide is mediated by mast cell serotonin release in the rat. Toxicology and Applied Pharmacology 1990: 104(3), 403-410.
Hepcidin
Liver
Decreases iron absorption in intestines
Decreases iron release by macrophages
Chronic inflammation causes elevated hepcidin, making iron less available. This is called anemia of chronic inflammation.
Weiss G. Anemia of chronic disorders: new diagnostic tools and new treatment strategies. Seminars in Hematology 2015: 52(4), 313-320.
Human chorionic gonadotropin (HCG)
Placenta
Maintains hormone release in ovaries during pregnancy
Inhibition of immune defense against fetus
Not known to directly affect mast cell activation or histamine release
Schumacher A, et al. Endocrine factors modulating immune responses in pregnancy. Front Immunol 2014: 5, 196.
Perpetuates immediate and late phase hypersensitivity reactions
H3 receptor activation inhibits dopamine production
Dopamine is released by mast cells
H1 inverse agonists increase dopamine release
Histamine increases dopamine release
Mori T, et al. D1-like dopamine receptors antagonist inhibits cutaneous immune reactions mediated by Th2 and mast cells. Journal of Dermatological Science 2013: 71, 37-44.
Xue L, et al. The effects of D3R on TLR4 signaling involved in the regulation of METH-mediated mast cell activation. International Immunopharmacology 2016: 36. 187-198.
Endothelin
Stomach
Promotes smooth muscle contraction of stomach
Very potent vasoconstrictor
Activates mucosal mast cells
Mast cells regulate endothelin levels to prevent loss of blood flow to tissues
Boros M, et al. Endothelin-1 induces mucosal mast cell degranulation and tissue injury via ETA receptors. Clin Sci (Lond) 2007: 103(48), 31S-34S.
Hultner L, Ehrenreich H. Mast cells and endothelin-1: a life-saving biological liaison. Trends Immunol 2005: 26(5), 235-238.
Epinephrine/ adrenaline
Adrenal gland (medulla), sympathetic nervous system
Fight or flight response
Increases heart rate, force of heart contraction, blood pressure, energy breakdown, production of ACTH, bloodflow and energy to the brain and muscles
Suppresses nonessential functions and significantly decreases GI motility and excretion of urine and stool
Epinephrine inhibits IgE mediated released of histamine, prostaglandins and TNF
Epinephrine inhibits mast cell proliferation, adhesion and movement within the body SCF reduces action of epinephrine on mast cells by decreasing B2 adrenergic receptors
Cruse G, et al. Counterregulation of beta(2)-adrenoceptor function in human mast cells by stem cell factor. J Allergy Clin Immunol 2010: 125(1), 257-263.
Scanzano A, Cosentino M. Adrenergic regulation of innate immunity: a review. Front Pharmacol 2015.
Erythropoietin
Kidney
Stimulate red blood cell production
Protects nerve cells and tissues
During low oxygen events, mast cells express receptors for erythropoietin
Erythropoietin can bind at the CKIT receptor
Decreases inflammatory response to infection (decreases IL-6 and TNF)
Wiedenmann T, et al. Erythropoietin acts as an anti-inflammatory signal on murine mast cells. Mol Immunol 2015: 65(1), 68-76.
Estradiol and other estrogens
Ovaries, placenta, adipose tissue, testes
Drive female secondary sex characteristics
Increase metabolism, uterine and endometrial growth, bone production, and the release of cholesterol in bile
Increase production of proteins in liver, cortisol, sex hormone binding globulin, somatostatin, clotting factors II, VII, IX, X, antithrombin III and plasminogen, HDL, triglycerides
Decrease LDL, production of adipose tissue, GI motility
Modulate salt and water retention
Inhibits programmed cell death of germ cells
E2 is a very potent mast cell degranulator
E2 drives mast cell degranulation in ovaries to trigger ovulation
Enhances IgE mediated degranulation
Increased production of leukotrienes
Increases mast cell density in ovaries
Zaitsu M, et al. Estradiol activates mast cells via a non-genomic estrogen receptor-a and calcium influx. Mol Immunol 2007: 44(8), 1977-1985.
Zierau O, et al. Role of female sex hormones, estradiol and progesterone, in mast cell behavior. Front Immunol 2012: 3, 169.
Follicle stimulating hormone (FSH)
Pituitary
Stimulates maturation of ovarian follicles
Stimulates maturation of seminiferous tubules, production of sperm and production of androgen binding protein
Triggers mast cell degranulation
Increases mast cell density in ovaries
Theoharides TC, Stewart JM. Genitourinary mast cells and survival. Transl Androl Urol 2015: 4(5), 579-586.
Jaiswal K, Krishna A. Effects of hormones on the number, distribution and degranulation of mast cells in the ovarian complex of mice. Acta Physiol Hung 1996: 84(2), 183-190.
Akiyama T, et al. Roles of glutamate, substance P, and gastrin-releasing peptide as spinal neurotransmitters of histaminergic and nonhistaminergic itch. Pain 2014: 155, 80-92.
TNF blockers like Enbrel and infliximab can lower depression independent of improvements with physical symptoms. 62% of patients with treatment resistant depression saw improvement on infliximab versus 33% with standard therapies. Infliximab also improved sleep, allowing patients to stay asleep longer. Infliximab successfully improved depression symptoms in patients with inflammatory disease as well as controls who had elevated CRP and TNF but not on controls with normal CRP and TNF. Patients who were not effectively treated with SSRIs were found to have higher IL-6 and TNF.
Chronic inflammation can cause structural and functional changes in the brain, interfering with its ability to make new connections and damaging existing function. Activation of microglial cells in the nervous system is associated with maladaptive behaviors and decreased brain function seen in bipolar disorder, major depressive disorder and other mood conditions. They also protect neurologic function in multiple sclerosis, Huntington’s and Alzheimer’s. Minocycline, an antibiotic, also has significant anti-inflammatory and neuroprotective effects.
In some encephalitis models, DMARDs can actually restore stem cells of the nervous system, reducing tissue and myelin damage. DMARDs, often used for autoimmune diseases, improve mood symptoms in rheumatoid arthritis patients. They can also mitigate hyperactivity from amphetamines. Clinical trials are currently investigating the full effects of these medications on psychiatric conditions.
Mood stabilizers often have anti-inflammatory effects. In bipolar disorder patients, lithium and valproate decreased IL-6. Medications that act on serotonin and dopamine receptors decrease production of inflammatory molecules like TNF, IL-6 and PGE2. Escitalopram, an SSRI antidepressant, can decrease cortisol production and IL-11. ACTH production can be induced by fluoxetine.
References:
Furtado M, Katzman MA. Examining the role of neuroinflammation in major depression. Psychiatry Research 2015: 229, 27-36.
Rosenblat JD, et al. Inflamed moods: a review of the interactions between inflammation and mood disorders. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2014; 53, 23-34.
I know a lot of people have been waiting with bated breath for the outcome of the trial assessing the use of midostaurin (PKC412) in advanced systemic mastocytosis (a term describing aggressive systemic mastocytosis, mast cell leukemia, and systemic mastocytosis with associated clonal hematologic non-mast cell lineage disease).
A press release described the outcome of the phase II trial. Read it here.
Data from the phase II trial was also published. Read it here.
Please note that because of my job, I cannot answer questions about this medication.
In some cases, glucocorticoids can immediately treat issues with immune activation. This immediate action is not well understood. In animal models, glucocorticoids can stop allergic reactions in five minutes and significantly decrease short term histamine release. Mostly though, glucocorticoids mitigate mast cell activation through delayed actions. This is one of the reasons why premedication with steroids prior to surgery or procedures is recommended to start the day before.
Glucocorticoids affect gene expression, which is one of the reasons they take time to work. Gene expression is very complicated and is highly regulated by cells. Genes are part of your DNA. Think of each gene as a message. When your cell wants to make something using a gene, like a protein, it makes a copy of the message in the gene and then takes it to another part of the cell to make the protein. There are many molecules that affect how easy it is to make something from a gene. Some molecules make it easier and others make it harder. Transcription factors are molecules that sit by genes that make it easier for their message to be made. Interfering with making the message and getting it to the part of the cell where it can make something, like the protein, can drastically alter the behavior of a cell.
One of the major ways that glucocorticoids interfere with making the message is with glucocorticoid receptors. Many people know that receptors are often on the outside of a cell and they are activated when a molecule fits into the receptor like a key into a lock. Glucocorticoid receptors do not work like that. They are small molecules inside cells that are changed when glucocorticoids bind to them.
Cortisol, or other glucocorticoids, bind to the glucocorticoid receptors inside mast cells. When this happens, they interfere with the transcription factors so it is really hard to use the genes. Some of these transcription factors are called NF-kB and AP-1. When glucocorticoid receptors have been activated in the mast cell, the transcription factors can’t help to use the genes.
Cytokines are molecules that cells use to “talk” to each other. Another kind of signal. Glucocorticoids directly interfere with use of cytokine genes so that they aren’t made. Mast cells make many cytokines and they are responsible for a lot of late phase allergic symptoms. Manufacture of IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-8, IL-10, IL-13, GM-CSF, TNF and IFN-g (interferon gamma) can all be suppressed with glucocorticoids.
If the cytokine genes have already been used, glucocorticoids can still prevent them from being made. When you use a gene to make something, it creates a messenger RNA (mRNA) that carries the message. If the mRNA falls apart, nothing will be made from the gene. Glucocorticoids make the messages fall apart before making anything for many cytokines, including IL-1, IL-2, IL-6, IL-8, TNF and GM-CSF.
References:
Oppong E, et al. Molecular mechanisms of glucocorticoid action in mast cells. Molecular and Cellular Endocrinology 2013: 380, 119-126.
Varghese R, et al. Association among stress, hypocortisolism, systemic inflammation and disease severity in chronic urticaria. Ann Allergy Asthma Immunol 2016: 116, 344-348.
Zappia CD, et al. Effects of histamine H1 receptor signaling on glucocorticoid receptor activity. Role of canonical and non-canonical pathways. Scientific Reports 2015: 5.
Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol Cell Endocrinol 2011: 335(1), 2-13.
Sinniah A, et al. The role of the Annexin-A1/FPR2 system in the regulation of mast cell degranulation provoked by compound 48/80 and in the inhibitory action of nedocromil. International Immunopharmacology 2016: 32, 87-95.
A number of inflammatory conditions coincide with mood disorders. Women with chronic health issues who pursue diagnosis are commonly labeled as having anxiety and the physical symptoms as a result of that. However, there is a significant body of evidence pointing to mood disorders as being organic symptoms of the inflammation rather than the psychological reaction to the changes that come with chronic illness. What we often frame as behavioral or psychiatric symptoms are perceived by some researchers as “sickness behavior” that promotes healing. Low energy, appetite and mood, along with sleeping more, redirect energy from less important functions to immune defense or wound repair.
Patients with autoimmune disease, diabetes, metabolic syndrome, asthma and allergies all experience mood disorders. Psoriasis dramatically increases the frequency of depressive symptoms. Cardiovascular disease patients are more likely to have major depressive disorder or bipolar disorder than the general population. Major depressive disorder increases risk of coronary artery and poorer prognosis with cardiovascular disease.
In one study with ISM and CM patients, 75% reported symptoms of depression. In a different study, 60% reported depressive symptoms and anxiety. Asthma and wheezing are independently associated with major depressive episodes in a massive study with almost 250,000 people from 57 countries.
Depression patients who have attempted suicide show increased TNF and IL-6, along with low IL-2, compared to depression patients who have not attempted suicide. Elevated CRP is also associated with depression. Alexithymia, in which the patient feels no emotions, affects 39-46% of patients with major depressive disorder. These patients also demonstrate very high CRP levels which can decrease cognitive functions.
Treatment of chronic illnesses can also improve associated mood disorders. Aspirin is currently being trialed as a treatment for bipolar disorder. Use of aspirin with an SSRI produced better response than just the SSRI. Use of COX-2 inhibitors like celecoxib with antidepressants improves symptoms and decreases levels of IL-6 and IL-1b. NSAIDs, which also interfere with COX-2, reduce depression when compared to placebo.
Omega-3 polyunsaturated fatty acids have been found to be potent antidepressants. These molecules also decrease the production of prostaglandins and cytokines. Omega-3 polyunsaturated fatty acids interfere with the COX-2 enzyme that produces prostaglandins. Curcumin also decreases cytokine production, as well as normalizing activity from the HPA axis and improving mood.
References:
Furtado M, Katzman MA. Examining the role of neuroinflammation in major depression. Psychiatry Research 2015: 229, 27-36.
Rosenblat JD, et al. Inflamed moods: a review of the interactions between inflammation and mood disorders. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2014; 53, 23-34.
Vitamin D is an essential fat soluble vitamin that functions as a hormone. Its primary function is to promote intestinal absorption of calcium, magnesium, phosphate, iron and zinc. It also has a variety of anti-inflammatory and immunoregulatory effects. Deficiency of vitamin D3 has been linked previously to a number of inflammatory conditions, like asthma, diabetes mellitus, eczema and other atopic disorders.
A significant portion of vitamin D is produced in the skin when exposed to sunlight. The precursor 7-dehydrocholesterol in the skin is changed to form cholecalciferol, vitamin D3, when irradiated with UVB light. In the liver, cholecalciferol (vitamin D3) is metabolized to form 25-dihydroxyvitamin D3. In the kidney, it is further metabolized to 1,25-dihydroxyvitamin D3. Vitamin D2 and D3 supplements may also be taken orally. They will be processed by the liver in a similar fashion. Vitamin D3 is much more active than vitamin D2.
Vitamin D3 can exert a number of effects on mast cells. Though the mechanism is unclear, vitamin D3 seems to regulate the action of COX, the enzyme that produces prostaglandins. Accordingly, vitamin D3 can disrupt prostaglandin production.
It interferes with the production of cytokines, and chemokines, including Il-1, IL-6, IL-33, and TNF. It inhibits release of IL-6 and CRP. It is thought that vitamin D affects the stability of the mRNA for these molecules. This means that the genes for these molecules are not being used appropriately and so they cannot be made.
Vitamin D3 can also induce production of anti-inflammatory mediators. IL-4 and IL-10 are mast cell mediators that regulate inflammation. Vitamin D3 is required for their production and release. IL-10 can mitigate inflammation resulting from IgE activation. A single application of vitamin D3 to the skin decreased the immediate skin response to an IgE allergen. It decreased production of leukotrienes and histamine. Mast cells have vitamin D receptors (VDRs) inside their cells and close to where the genes are stored. Mast cell VDRs must be present to see these effects.
Long term use of vitamin D3 (30-40 days) was found to cause mast cell apoptosis (programmed cell death) in a cell model. Vitamin D3 also directly impeded the differentiation and maturation of mast cell precursors.
There is a lot we do not know about how vitamin D3 interacts with mast cells but it is generally considered to have an anti-inflammatory and anti-allergic effect.
References:
Yip KH, et al. Mechanisms of vitamin D3 metabolite repression of IgE-dependent mast cell activation. Journal of Allergy and Clinical Immunology 2014: 13395), 1356-1364.e14
Conti P, Kempuraj D. Impact of vitamin D on mast cell activity, immunity and inflammation. Journal of Food and Nutrition Research 2016: 4(1), 33-39.
Glucocorticoids, like cortisol, can affect mast cells in many ways. As I discussed in my previous post, there are many ways for mast cells to release mediators when activated. In all of these pathways, there are many molecules involved that carry the signal, like people passing the Olympic torch. In mast cells, one of the molecules that suppresses inflammatory activation signal is called SLAP (yes, really). Cortisol increases the amount of SLAP in mast cells so inflammatory activation signals are suppressed.
An important step in degranulation is changing the amount of calcium inside the cell and moving it to different parts of the cell. In some studies, glucocorticoids can affect this movement of calcium. Other studies have found that in some pathways, glucocorticoids don’t affect calcium movement, but instead interfere with things like the IgE receptor.
Cortisol is also thought to directly inhibit stem cell factor (SCF) binding to the CKIT receptor. When SCF binds to the CKIT receptor, this sends a signal to the mast cell to stay live. This means that taking glucocorticoids can let mast cells die at the appropriate time. SCF also tells mast cells to go to inflamed spaces. By blocking this signal, glucocorticoids suppress inflammation.
One of the ways that molecules carry a signal is by changing the next molecule in the pathway. A big way that cells changing molecules is by chopping off a piece of them called a phosphate group. This is done by special enzymes called phosphatases. Glucocorticoids affect the availability of phosphatases so they aren’t able to get to the right part of the cell to carry the signal. When this happens, there is less activation and less histamine release.
Arachidonic acid is the molecule modified to make eicosanoids (leukotrienes, thromboxanes and prostaglandins.) Glucocorticoids directly interfere with the production of these molecules in multiple ways. The first way is by interfering with COX-2, one of the enzymes that makes prostaglandins. Another way is by preventing arachidonic acid from being released to a place where they can be turned into leukotrienes, thromboxanes and prostaglandins. This occurs because glucocorticoids increase the amount of a powerful anti-inflammatory molecule called annexin-I. Annexin-I inhibits the molecule that releases the arachidonic acid, called phospholipase A2.
Annexin-I was the subject of an important paper earlier this year. In trying to identify exactly how mast cell stabilizers like ketotifen and cromolyn work, the researchers discovered that treatment with mast cell stabilizers decreased degranulation and increased annexin-I made by mast cells. They also found that glucocorticoids had the same effect.
References:
Oppong E, et al. Molecular mechanisms of glucocorticoid action in mast cells. Molecular and Cellular Endocrinology 2013: 380, 119-126.
Varghese R, et al. Association among stress, hypocortisolism, systemic inflammation and disease severity in chronic urticaria. Ann Allergy Asthma Immunol 2016: 116, 344-348.
Zappia CD, et al. Effects of histamine H1 receptor signaling on glucocorticoid receptor activity. Role of canonical and non-canonical pathways. Scientific Reports 2015: 5.
Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol Cell Endocrinol 2011: 335(1), 2-13.
Sinniah A, et al. The role of the Annexin-A1/FPR2 system in the regulation of mast cell degranulation provoked by compound 48/80 and in the inhibitory action of nedocromil. International Immunopharmacology 2016: 32, 87-95.
There are many ways for mast cells to be activated. Each of them involves a sequence of events involving several molecules. These molecules change the next molecule in line in a way that causes it to perform a specific action. It is hard to visualize and one of the harder concepts to understand about molecular biology.
I think of it like carrying the Olympic Torch to the Olympic Games. Before the Olympic Games, the Olympic Torch is lit in Greece. Then a series of different people from all over the world carry the torch part of the way before giving it to another person. Many, many people are involved, and the environment changes, but the torch always stays lit. Finally, the very last person carries the torch into the stadium to light the Olympic Flame to open the Olympics. Even though the people and environment changed, it’s still the same flame.
In the body, pathways are just like passing this Olympic torch. Instead of people carrying the flame and keeping it lit, molecules carry a message that they tell to the next molecule, and so on until the pathway ends. The best known mast cell activation pathway is IgE activation. IgE binds to a receptor on the outside of the mast cell. The receptor knows that this means it has to degranulate. It passes this message to a molecule, which passes the message down the line, just like the torch, until the mast cell degranulates.
Mast cells are well known for having many large granules that hold mediators until there is a signal to release. Granules are like pockets and mast cells stuff them full of premade mediators like histamine and tryptase. Mast cells actually sort mediators so that the granules are organized and mediators aren’t distributed randomly. The way mediators are stored together greatly affects the action of these molecules once they are released.
Large scale degranulation (sometimes called complete or anaphylactic degranulation) is the best known mast cell mediator release mechanism. In this kind of degranulation, granules swell and then lots of granules actually clump together to make a very large pocket. Then, this super pocket goes to the edge of the mast cell, the cell membrane, and pokes a hole to the outside. The mediators in the super pocket are then released at once. The granules and membrane have holes in them that will eventually be repaired. Following large scale degranulation, it takes about two days for normal mast cells to regranulate.
There is another kind of degranulation called piecemeal degranulation. This involves release of some mediators in a granule. There is still a lot we don’t know about this process, but the general idea is that a regular granule puts some of its mediators into a tiny little bubble. The little bubble then goes to the edge of the mast cell and slowly releases these mediators. In piecemeal degranulation, the granules do not clump together to make one large granule, and there is no hole made in the membrane. It is believed that some molecules help to push the mediators out of the cell but we don’t know what they are.
A number of mast cell mediators are not stored in granules and are instead made upon signals from specific pathways. Because these molecules aren’t stored in granules, it takes some time for them to be produced and released after mast cell activation. Lipid mediators, like prostaglandins and leukotrienes, are packed together and then transported across the membrane to the outside by other molecules. Cytokines and chemokines are also produced on demand and then stored in small bubbles. These small bubbles are then actively pushed out of the cell in a process called exocytosis.
References:
Moon TC, et al. Mast cell mediators: their differential release and the secretory pathways involved. Front Immunol 2014: 5:569.
Wernersson S, Pejler G. Mast cell secretory granules: armed for battle. Nat Rev Immunol 2014: 14(7), 478-494.
Author’s note: I am not a medical doctor. Anaphylaxis and use of epinephrine must be discussed with the managing provider to determine the best treatment plan for any individual patient.
Determination of mast cell reaction vs anaphylaxis
Anaphylaxis has a very complicated relationship with mast cell disease. Mast cell symptoms and reactions are inherent parts of mast cell disease. All mast cell patients can reasonably expect to have some mast cell symptoms as part of their baseline.
Anaphylaxis is not an inherent part of mast cell disease. Anaphylaxis is a complication of mast cell disease. Mast cell patients are at increased risk for anaphylaxis, but not all mast cell patients experience anaphylaxis. In some studies, as many as 50% of mast cell patients had never experienced anaphylaxis.
The fact that anaphylaxis and mast cell reactions can have the same symptoms is probably the reason why it is difficult to separate the two. So for a minute, let’s stop talking about mast cell disease and consider a similar scenario that is better described.
Coronary artery disease (CAD) is the leading cause of death worldwide. It affects millions of people around the world. Everyone knows someone with coronary artery disease. Probably multiple someones.
Patients with CAD have narrow arteries that interfere with blood flow to the heart. When they are diagnosed with CAD, their provider will tell them about symptoms they may experience daily as a normal part of their disease. Their provider will also tell them about symptoms that they may experience that indicate the heart is not getting enough oxygen, like radiating chest pain, shortness of breath and nausea. In these scenarios, the patient needs to take a med like nitroglycerin to try and stop the episode. If that doesn’t work, the patient is at risk for a heart attack.
Radiating chest pain, shortness of breath and nausea are symptoms of CAD. Heart attack is not a symptom of CAD. It is a complication of CAD. It can also present with the same symptoms of radiating chest pain, shortness of breath and nausea.
Flushing, nausea, diarrhea and hives are symptoms of mast cell disease. (I’m just using these as examples, there are many others). Anaphylaxis is not a symptom of mast cell disease. It is a complication of mast cell disease. It can also present with the same symptoms of flushing, nausea, diarrhea and hives.
These are the potential scenarios when a mast cell patient starts experiencing more severe symptoms than usual.
The patient experiences flushing, nausea, diarrhea and hives. They don’t take rescue meds and the symptoms resolve. This is a mast cell reaction. This is not anaphylaxis.
The patient experiences flushing, nausea, diarrhea and hives. They take rescue meds (not including epi here) and the symptoms resolve. This is a mast cell reaction. This is not anaphylaxis.
The patient experiences flushing, nausea, diarrhea and hives. They may or may not take rescue meds (not including epi here). Either way, the symptoms do not resolve. The amount of mast cell degranulation triggers a large scale reaction that initiates anaphylaxis. This is anaphylaxis and requires epinephrine. There are two possibilities here: it was anaphylaxis from the beginning, or it started as a mast cell reaction and became anaphylaxis. Either way, it requires epinephrine and other rescue meds.
It seems to me that when anaphylaxis occurs in mast cell patients as a sudden onset event that the symptoms seen are usually distinct from regular mast cell reaction symptoms. (This last sentence is based upon what I have experienced and what is reported to me by patients. There is no data on this.)
General notes on use of epinephrine
How do you know it is anaphylaxis? That’s the hard part. Mast cell experts feel differently about this. Most say to only use epi if you have trouble breathing or low blood pressure because then you know it is life threatening and thus anaphylaxis and not a mast cell reaction.
If you are having trouble breathing or low blood pressure (for adults, under 90 systolic), that is generally cited as the appropriate point to use epi. However, it is a conversation and decision that must be made with you and a doctor that knows you and your disease.
If you have had an episode before where you had severe symptoms and recovered without epinephrine, it is phenomenally unlikely that it was anaphylaxis.
If you think you may need epinephrine and are unsure, it is generally recommended to use your epipen. The reason for this is that epinephrine is pretty safe, despite how the movies depict it. The risk of using an epipen when you don’t need it is side effects of epinephrine use: rapid heartbeat, elevated blood pressure, anxiety, and generally not feeling great for a day or so. The risk of not using an epipen when you need it is death. People die from anaphylaxis with their epipens on them unused.
Meeting diagnostic criteria for anaphylaxis
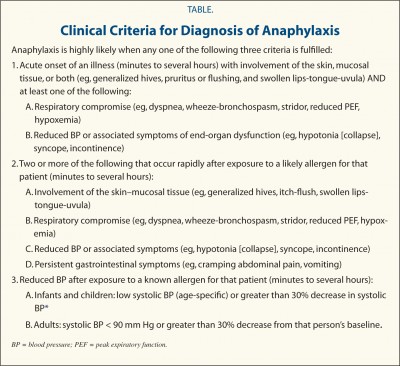
As I reviewed in the previous post, there are many sets of diagnostic criteria for anaphylaxis. The one that is the most widely used in the WAO criteria published in 2006. This set of criteria has been validated, meaning it was effective for correctly identifying patients experiencing anaphylaxis while excluding those who weren’t. Even still, they note that about 5% of patients with anaphylaxis will not be covered by these criteria and to use discretion with this population.
The 2006 WAO criteria (shown below) are often used by emergency departments to determine whether or not epinephrine is needed. If the patient meets the criteria, epi is warranted. This is one of the reasons why anaphylaxis is often considered synonymous with requirement of epinephrine.
2006 WAO Anaphylaxis Criteria
Determining whether or not you have anaphylaxis when your blood pressure is not very low and you can breathe fine is not straightforward for mast cell patients. There are several charts that are often posted in mast cell groups that show four or five stages of anaphylaxis. These charts are designed for people who do not have baseline allergic symptoms. Mast cell patients have baseline allergic symptoms.
If you have mast cell disease and have flushing, nausea and hives regularly, that is not grade II anaphylaxis. That is mast cell disease. Symptoms that are part of your normal baseline or reaction profile do not contribute to the overall assessment of anaphylaxis. So let’s assume I have flushing, nausea and hives every day. But then one day I also have diarrhea and tachycardia, which isn’t normal for me. That is grade III anaphylaxis per the Ring and Messmer scale (shown below). Whether or not you use epi at that point, assuming your blood pressure is not low and you can breathe okay, depends upon whether or not your doctor endorses the use of that scale.
Ring and Messmer Anaphylaxis Grading Scale
Anaphylaxis vs anaphylactic shock
I often see people use anaphylaxis and anaphylactic shock interchangeably. They’re not the same thing.
Anaphylaxis is a severe, multisystem allergic reaction.
Shock is more properly called circulatory shock. It is a state arising from poor circulation such that tissues are not receiving sufficient blood supply. Weak pulse, tachycardia, low heart rate, and mental status changes including loss of consciousness are all symptoms of shock.
Anaphylactic shock is circulatory shock caused by low blood pressure due to the vasodilation from large scale degranulation. By definition, it is blood pressure 30% below the patient’s baseline or below standard values (90 systolic for adults). So if you aren’t experiencing circulatory shock, you aren’t having anaphylactic shock.
References:
Sampson HA, et al. Second symposium on the definition and management of anaphylaxis: summary report – Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 2006: 117(2), 391-397.
Brown, SGA. Clinical features and severity grading of anaphylaxis. Journal of Allergy and Clinical Immunology 2004: 114(2), 371-376.
Sampson HA, et al. Symposium on the definition and management of anaphylaxis: summary report. J Allergy Clin Immunol 2005; 115(3), 584-591.
Ring J, et al. History and classification of Anaphylaxis. Chem Immunol Allergy 2010: 95, 1-11.